

Billing and Coding Guides
January 7, 2019PCMH Congress 2018 Highlights
January 23, 2019Using ICD-10 Asthma Severity CodesJanuary 2019 Newsletter
New York City is one of the top twenty “Asthma Capitals” in the United States, a designation based on asthma prevalence, asthma-related emergency visits, and asthma-related fatalities.i The City also has the third highest rate of asthma-related deaths in the country.ii
Data on provider documentation practices can inform new population health and clinical approaches to improving patient outcomes. The Evaluation, Research and Analysis team at the Primary Care Information Project (PCIP) reviewed the documentation of asthma severity in pediatric and adult patients. The findings present an opportunity to improve asthma severity documentation, which is important for patient treatment, targeted interventions, and claims reporting.
Reviewing Asthma Severity Documentation
Using data from aggregate electronic health records (EHR), the team reviewed the use of ICD-10 codes to document the specificity of a patient’s asthma condition. Under the expanded ICD-10, coding allows for asthma diagnoses to be classified by severity with greater specificity. Aggregated data were limited to the number of patients who visited a provider in 2016 and had an ICD-10 asthma code in their problem list or assessment. A total of 619 practices, accounting for 1.7 million patients, contributed data.
Findings
The most commonly selected asthma diagnosis codes were “unspecified” and “other.” These two codes were used twice as often as any of the more specific ICD-10 severity codes. Of the patients, 7.2 percent had an asthma diagnosis, but only half of those patients had a diagnosis that specified the severity of their condition. The findings show that severity codes were used less for adult patients than for pediatric patients, even though asthma is typically more severe in adults (adults are four times more likely than children to die from asthmaiii). “Mild intermittent” was the most commonly used severity code across all practice types and patient demographics. Pediatric practices were more likely to use severity codes than other practice types.
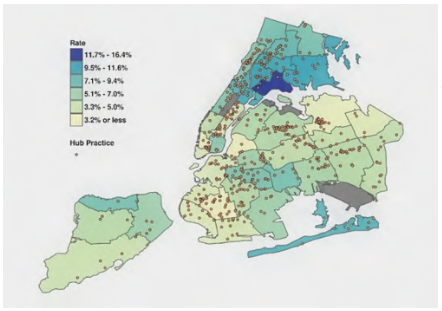
Asthma Diagnosis by UHF neighborhood
The data show a similar pattern to previous findings on the distribution of asthma in New York City: the South Bronx (16.4%) and East Harlem (10.8%) are asthma hotspots, and children aged 5 to 11 had the highest prevalence of any age group (12.8%).
Importance of Using ICD-10 Severity Codes
Detailed documentation of asthma severity may lead to improved patient outcomes. Knowing the severity of asthma is an important indicator for treatment and management. Using ICD-10 severity codes can help better manage patients’ asthma and prevent avoidable hospitalizations and emergency room visits.iv Communicating this information to patients helps them understand their own condition, and documenting severity is useful to other care providers who may be unfamiliar with a patient’s medical history. The use of severity codes can also help identify patients with severe or poorly managed asthma and, in turn, public health or health systems can develop more targeted, effective population-based interventions.
The codes used in documentation for disease severity impact provider’s evaluation of care and related reimbursements. The use of unspecified codes may result in payment delays and unnecessary claim denials by the Centers for Medicare & Medicaid Services (CMS) and other payers. CMS requires the use of 5th or 6th character placement to report the highest level of specificity (for asthma and for other conditions).v
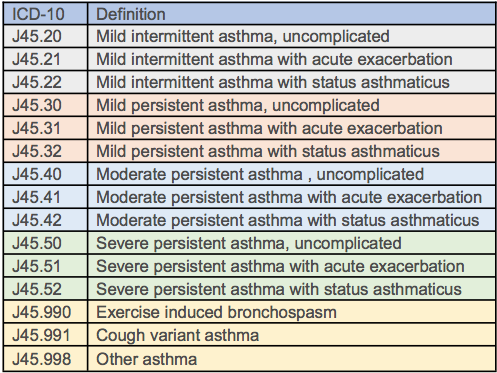
Codes follow National Asthma Education and Prevention Program guidelinesvi
Guidance on Using ICD-10 Severity Codes
Aggregated information from over 600 practices suggests that the low usage of ICD-10 severity codes may be the result of issues accessing codes in EHR systems. For example, several providers did not know to use the severity codes because their EHR system was not fully updated.
The table to the right lists ICD-10 codes available for specifying asthma severity. Providers should be able to see all of these codes and select any of them in their EHR. If not, providers should contact their EHR vendor.
Consider taking a few minutes to review clinical documentation and ensure codes align with the severity documented in the patient’s health record.
For a step-by-step guide to updating and mapping ICD, CPT, and LOINC codes in eClinicalWorks, watch the Electronic Health Record Tips & Tricks webinar on the NYC REACH resource library at www.nycreach.org (Electronic Health Record Assistance folder).
Please contact pcip@health.nyc.gov for further assistance.
Contributing Research Staff
Emily Martinez, MPH; Jenny Smolen, MPH; Charlene Ngamwajasat, MD; Katherine Kaye, MD; Sachin Jain, MD, MPH; Samantha De Leon, PhD; Sarah Shih, MPH.
References
i. Asthma Capitals 2018. Asthma and Allergy Foundation of America. http://www.aafa.org/media/AAFA-2018-Asthma-Capitals-Report.pdf. Accessed November 2018.
ii. Asthma Capitals 2018. Asthma and Allergy Foundation of America. http://www.aafa.org/media/AAFA-2018-Asthma-Capitals-Report.pdf. Accessed November 2018.
iii. Asthma Facts and Figures. Asthma and Allergy Foundation of America. http://www.aafa.org/page/asthma-facts.aspx. Accessed November 2018.
iv. Asthma Care Quick Reference. U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/files/docs/guidelines/asthma_qrg.pdf. Accessed November 2018.
v. 2019 ICD-10-CM. Centers for Medicare & Medicaid Services https://www.cms.gov/Medicare/Coding/ICD10/2019-ICD-10-CM.html . Accessed November 2018.
vi. Asthma Care Quick Reference: Diagnosing and Managing Asthma. U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/files/docs/guidelines/asthma_qrg.pdf. Accessed November 2018.